Category Archives: Uncategorized
Funding for C3FIT Trial Approved by PCORI
Recently, the board of PCORI approved funding for the Comparative Effectiveness Randomized Trial to Improve Stroke Care Delivery: C3FIT: Coordinated, Collaborative, Comprehensive, Family-Based, Integrated, and Technology-Enabled Care. The PCORI summary is here. I’m pleased to be serving on the stakeholder engagement committee for the study.
Diminishing returns in medical therapy
I’m a few months late, but I want to mention an editorial by Rodney Hayward that was published in The BMJ in December 2015. His topic is treatment of diabetes, but the principles he discusses also apply to other areas of medicine. The key concept is that even in high risk conditions such as diabetes, adding a second or third medication brings diminishing absolute returns as residual risk decreases as each additional treatment is added. He starts by describing the disturbing consequences of untreated or poorly managed diabetes, and how things have changed with modern therapies.
When I began my medical training in 1980, I commonly encountered patients whose bodies were ravaged by end stage complications of diabetes. These patients often had marked visual impairment, debilitating neuropathy, myopathies, and diabetes related renal insufficiency, well before age 65 years. I still occasionally see such individuals, but they are rare, and tend to come from the 10-15% of patients who still have poor glycemic control. Improvement in diabetes care is a medical success story, but increasing evidence suggests that overly aggressive treatment is an under-appreciated problem.
The problem is that focusing on relative treatment effects ignores the law of diminishing returns; past a certain point, additional reductions in HbA1c have limited benefit in absolute terms for most older patients with type 2 diabetes. Hayward explains:
Diminishing returns is a mathematical fact, not a theory. Try this simple experiment. Serially tear a piece of paper in half and throw one half away. You will notice that the relative effects never diminish (you reduce the piece of paper by half each time), but it doesn’t take long for the 50% you throw away to become tiny. The many patients with end stage diabetes we saw in the 1980s often spent years with poor control of both glycemia and blood pressure. They had no access to metformin, home blood glucose monitoring, angiotensin converting enzyme inhibitors, calcium channel blockers, and a host of other modern interventions. Each of these interventions substantially reduces disease progression and has an even larger effect on end stage diabetes complications. Because each intervention substantially reduces end stage complications, it should not be surprising that recent evidence has found intensive glycemic control to have a small absolute effect on end stage complications for most patients with type 2 diabetes. The law of diminishing returns predicts this result. Also, as the benefits of tighter glycemic control become smaller, the chances that treatment harms will outweigh treatment benefits become much greater.
Hayward ends by stating that the public good would best be served by focusing on the minority of diabetes patients who continue to be at substantial risk of diabetes-related morbidity and mortality and promoting more shared decision making with older diabetes patients who already have at least moderate blood glucose control.
The same principle of diminishing returns applies in other areas of medicine, such as in medications that reduce cardiovascular risk by lowering blood pressure or cholesterol. As the second and third medication is added, the patient’s risk of experiencing a cardiovascular event diminishes and in some cases a point can be reached where the absolute benefits become very small and it becomes difficult to tell whether benefits outweigh harms. When benefits become small, it can sometimes be hard to determine whether they exist at all or, perhaps, exist in only in patients with certain characteristics. See this post by Harlan Krumholz for a discussion of these issues in the area of treatment of high blood pressure.
In the area of cholesterol-lowering drugs, the new PCSK9 inhibitors have been in the news and I’ve previously discussed them on this blog (here, here and here). Two of these drugs, evolocumab and alirocumab, are approved in the U.S. and so far aren’t selling well. There are several reasons for that, including that the outcomes trials haven’t been completed yet and that the drugs are much more expensive than statins, almost all of which are available as generics. Another reason, related to the first two, is that insurance companies have imposed strict preauthorization requirements for these drugs. Another reason relates to the theme of this post, namely the diminishing returns from adding additional drugs. I’m going to take the treatment of heterozygous familial hypercholesterolemia (HeFH) as an example, specifically patients with HeFH who do not have clinical atherosclerotic cardiovascular disease and who are thus being treated to prevent a first event (i.e., “primary prevention”).
HeFH greatly increases the risk of developing premature atherosclerotic cardiovascular disease compared to individuals with normal levels of cholesterol. Before statins became available, the drugs that were available were not very effective. However, in recent decades, first moderate intensity and then high intensity statins were instituted as standard treatment of HeFH, often with additional drugs such as ezetimibe. According to UpToDate, atorvastatin can reduce LDL by up to 54% and rosuvastatin can reduce LDL by up to 63%. Ezetimibe can lower LDL by another 15% or so in patients on a statin. Given that most patients with HeFH have LDL in the 200s or below, a reduction of 50-60% achieves very reasonable LDL levels. There is evidence that even moderate doses of statins greatly reduce the risk of heart disease in HeFH patients who are being treated for primary prevention. A study published in JAMA in 2014 showed that young adults with HeFH have near-normal levels of atherosclerosis 10 years after initiation of statin therapy. The use of high intensity statins has been shown to greatly reduce the progression of atherosclerosis in adult HeFH patients (see here and here) even when compared to moderate statin therapy. Thus, HeFH patients who start treatment early and are able to reduce their LDL to normal or near-normal levels over many years with a statin or statin + ezetimibe often do not need an additional drug, as their risk is greatly reduced.
So which HeFH patients do need an additional LDL-lowering therapy, such as a PCSK9 inhibitor? To my knowledge, there are no risk calculators available to guide decisions in this area. HeFH patients who start with very high LDL, who can’t tolerate high doses of statins or can’t tolerate statins at all, who started treatment late, who have additional cardiovascular risk factors, or who have had imaging that shows significant subclinical atherosclerosis, are going to be at higher risk, on average. There is quite a bit of uncertainty involved, as with estimation of cardiovascular risk in general. In addition, there are personal preferences involved, as people vary greatly in terms of how much risk they are willing to live with.
Interestingly, a task force of the International Atherosclerosis Society just published a consensus statement in The Lancet Diabetes & Endocrinology that discusses some of the factors involved in determining cardiovascular risk in FH. Although the criteria they propose for use of additional therapies are more stringent than I foresee being adopted in the U.S., the paper contains some very useful discussion of the heterogeneity of cardiovascular risk in FH and ways of trying to predict who is at higher risk. I’m pasting in their proposed criteria below, in case anyone is interested, but I do recommend the entire paper.

Third Annual PharmedOut Conference
PharmedOut, a Georgetown University Medical Center-based pharmaceutical marketing research project, hosts its third annual conference focusing on the misinformation and patient harm that can occur from pharmaceutical and medical device marketing.
WHO:
- Rita Redberg M.D., M.Sc., Archives of Internal Medicine Editor-in-Chief; professor of medicine, University of California, San Francisco
- Carl Elliott M.D. Ph.D., author, White Coat, Black Hat; professor, University of Minnesota’s Center for Bioethics
- Kay Dickersin Ph.D., director, Center for Clinical Trials, Johns Hopkins Center for Global Health
- Julie Taitsman M.D., J.D., chief medical officer, Office of the Inspector General, U.S. Department of Health and Human Services
- Sharon Treat J.D., executive director, National Legislative Association on Prescription Drug Prices
- Joel Lexchin M.D., professor, York University
- Donald Light Ph.D., professor, University of Medicine and Dentistry of New Jersey
For more information and to register, visit the PharmedOut conference page.
WHEN: Thursday, June 14 and Friday, June 15, 2012, 8:00 a.m. to 5:30 p.m. ET.
Thursday morning: Marketing of antipsychotic medications and other drugs
Thursday afternoon: Potential health risks of CT scans and other medical devices
Friday morning: Legislative and regulatory updates and solutions
Friday afternoon: Informing and protecting patients: The role of industry, media, and payers
WHERE: Lohrfink Auditorium in the Hariri Building, Georgetown University, 37th and O Streets, N.W., Washington, D.C., 20057.
“Choosing Wisely” campaign launched
The ABIM Foundation has joined with nine medical specialty societies to develop evidence-based lists of tests and procedures for patients and physicians to discuss and question. The goal of Choosing Wisely is to help physicians, patients and other stakeholders avoid unnecessary and in some cases harmful interventions and reduce the ever-expanding cost of health care. Each participating specialty society will identify five tests or procedures whose use should be questioned. The lists will be announced in April 2012. The lists are modeled after the National Physicians Alliance project “Five Things You Can Do in Your Practice,” which was funded by the ABIM Foundation. Consumer Reports will also be participating in the campaign. One page factsheet here. Press Release here. Website here.
10 steps to better risk communication
Every day, patients are faced with difficult medical decisions. These decisions invariably involve tradeoffs between risks and benefits. However, these risks and benefits are often not communicated in a way the patient can understand, if they are communicated at all. In a commentary in the Journal of the National Cancer Institute, Angela Fagerlin and colleagues highlight 10 methods that have been shown to improve understanding of risk and benefit information. Their commentary uses examples relating to cancer screening, prevention, and treatment, but the principles should apply in other areas. Below I summarize the key points; the authors state that the first three recommendations are based on strong evidence, while the rest are based on preliminary evidence.
- Communicate using “plain language.” According to the authors, the average American reads at an 8th grade level, but health education materials are often written at a high school or college level, making the information hard for the average person to understand.
- Present statistical information using absolute risk rather than using relative risk or number needed to treat formats. Changes in risk appear larger when presented using relative risk rather than absolute risk. Absolute risk is easier for most people to understand than number needed to treat.
- Use pictographs when possible when presenting information graphical format. The authors state that pictographs are easier to understand than other types of graphs, such as bar graphs and pie charts.
- Present data using frequencies rather than percentages. “10% of patients get a bad rash” and “10 out of a hundred patients get a bad rash” mean the same thing, but percentages are more abstract and/or harder to understand for some people.
- When discussing treatment complications or side effects, differentiate between baseline risks and incremental risks. Baseline risks are risks the person would face without any treatment; incremental risks are the risks associated with treatment. For example, an initial pictograph could show baseline risk and a second pictograph could add a new color to represent the additional people who would experience the side effect as a result of the treatment.
- Be aware that the order of presenting risks and benefits can alter risk perceptions. For example, if the benefits are presented first and the risks second, the risks may be perceived to be more worrisome and common. This issue can’t be avoided altogether, but can be minimized by summarizing all the information at the end.
- When there are numerous risks and benefits, use a summary table. Many treatments have numerous risks and benefits. It is easier to compare the risks and benefits if they are presented in a summary table.
- Recognize that comparative risk information can bias decision making by altering how a person views his or her own risk. If a person is given information indicating that their risk of developing a disease is higher than average, they may be more likely decide in favor of an intervention. Decisions should be based on whether the benefits of the intervention outweigh its risks for an individual person, which can only be decided based on absolute risk.
- Consider that providing less information may be more effective. Presenting more information can distract people from focusing on the key pieces of information that are needed for decision making.
- Make clear the time interval over which a risk occurs (e.g., 5-year risk, 10-year risk, 20-year risk).
I recommend reading the entire commentary. If you don’t have access to the PDF, email me and I will send it to you.
Pharma and patients
Thanks to Gary Schwitzer for interviewing me on his blog. The topic is the intersection of pharma, patients and social media.
Conference to discuss pharma influence on medical knowledge
A conference, “Pharma Knows Best? Managing Medical Knowledge,” will be held June 16-17, 2011 at Georgetown University in Washington, DC. Topics to be covered at the conference include ghostwriting and medical journals; academic-industry-relationships; disease awareness sites and social media, pharmaceutical benefits managers, targeting physicians through medical science liaisons, the role of the FDA in direct-to-consumer marketing of pharmaceuticals; and an analysis of the data from the Massachusetts gift-ban legislation.
Flyers for posting are available here. Here’s the registration site:
Here is the agenda:
Thursday, June 16, 2011
Moderator – Dennis McIntyre MD, Georgetown University Hospital
8:15am-9:00am The History of Academic-Industry Research Relationships
Nicholas Rasmussen PhD MPH, University of New South Wales
9:00am-9:30am Managing Medical Knowledge in a Market for ‘Lemons’
Donald Light PhD MS, UMDNJ, Stanford University
10:00am-11:00am Industry Relationships with Medical Journals
Marcia Angell MD, Harvard Medical School
Virginia Barbour MD, PLoS Medicine
11:00am-11:30am Publication Planning and Ghostwriting
Alastair Matheson PhD MSc, Toronto, Canada
11:30am-12:00pm Q&A/Discussion with Morning Speakers
Moderator – Tony Scialli MD, Tetra Tech Sciences, G.W. University School of Medicine
1:30pm -2:00pm DTC Promotion: The Role of FDA
Amy Toscano PharmD CPA, FDA-DDMAC
2:00pm -2:30pm How to do Pharma-free CME
Peter Brodhead, Memorial Sloan-Kettering Cancer Center
3:00pm-5:00pm Panel: Medical Education
Steve Willis MD, East Carolina University
Arnold Relman MD, Harvard Medical School
Joel Lexchin MD MSc, York University, University of Toronto
Friday, June 17, 2011
8:00am – 8:45am Disease Awareness Sites and Social Media
Jeff Chester MSW, Center for Digital Democracy
8:45am – 9:15am Framingham Cardiac Risk Calculation – A Case Study in Commercialization of the Digital Landscape
Jesse Polansky MD MPH, Baltimore, MD
9:15am – 10:00am Adherence and Compliance Programs, E-Sampling, and Other Marketing Platforms
Adriane Fugh-Berman MD, Georgetown University Medical Center
Moderator – Sharon Radzyminski PhD JD RN, Georgetown University School of Nursing and Health Studies
10:30am – 11:00am Universal Influence: An Analysis of the Data from the Massachusetts Gift-Ban Legislation
Elissa Ladd PhD RN FNP-BC, MGH Institute of Health Professions
11:00am – 11:30pm Pharmaceutical Benefits Managers
Mark Helm MD MBA, Helm Benefit Design
11:30pm-12:00pm Targeting Physicians through Medical Science Liaisons
Douglas Melnick MD MPH, Los Angeles, CA
12:00pm – 12:30pm Q&A/Discussion – Morning speakers
Moderator – Shannon Brownlee MS, New America Health Policy Program
1:30pm – 2:00pm What’s happening at Academic Medical Centers?
Susan Chimonas PhD, Institute on Medicine as a Profession
2:00pm – 2:30pm Academic Scientists’ Relationships with Industry
Eric Campbell PhD, Harvard Medical School
2:30pm – 3:00pm Prevalence of Academic-Industry Research Partnerships
Adriane Fugh-Berman MD, Georgetown University Medical Center
3:30pm – 4:00pm Should Academic Medical Centers Perform Industry Research?
Carl Elliott MD PhD, University of Minnesota School of Medicine
4:00pm – 5:00pmPanel/Discussion: Should Academic Medical Centers be Pharma-Free? Can Academic Medical Centers be Pharma-Free?
Edmund Pellegrino MD, Kennedy Institute of Ethics, Georgetown University
Marcia Angell, MD, Harvard Medical School
Heather Pierce JD MPH, AAMC
Curt Furberg MD PhD, Wake Forest University, North Carolina
The conference is sponsored by PharmedOut. Hope to see you there.
Editorial warns health organizations to avoid partnerships with Big Food
Highly processed, calorie-rich food is heavily marketed, highly profitable, and is one of the major causes of skyrocketing rates of child and adult obesity. The ubiquity of such foods in our society is said to create an “obesogenic environment.” So should the American Academy of Family Physicians accept a large grant from the Coca Cola Company to fund a consumer nutrition education website? Should the Heart and Stroke Foundation raise funds by selling pizzas from Boston Pizza? A hardhitting editorial by Yoni Freedhoff and Paul Hébert in the Canadian Medical Association Journal enumerates the benefits to food companies, and the risks to health organizations, in entering into such partnerships.
- For the food industry, partnerships with health organizations buy credibility and consumer loyalty.
- In many cases, partnerships with health organizations directly increase sales, as when Yum! Brands partnered with Susan G. Komen for the Cure to sell buckets of fried chicken.
- Such partnerships may help leverage corporate lobbying efforts, as when Coca-Cola’s CEO used the company’s alliance with AAFP to help argue that soda taxes were unnecessary.
- Although the obesity epidemic is primarily fueled by the consumption of excess calories, these partnerships are used by the food industry to promote the misleading message that inactivity, rather than its products, is the main cause of obesity.
The authors conclude that health organizations, even when desperate for money, should avoid partnering with the food industry. The editorial and an appendix enumerating examples of partnerships between the food industry and health organizations are freely available, so I urge you to read them in their entirety.
See comments by my fellow bloggers Larry Husten, Gary Schwitzer and Howard Brody. Hat tip to Yoni Freedhoff.
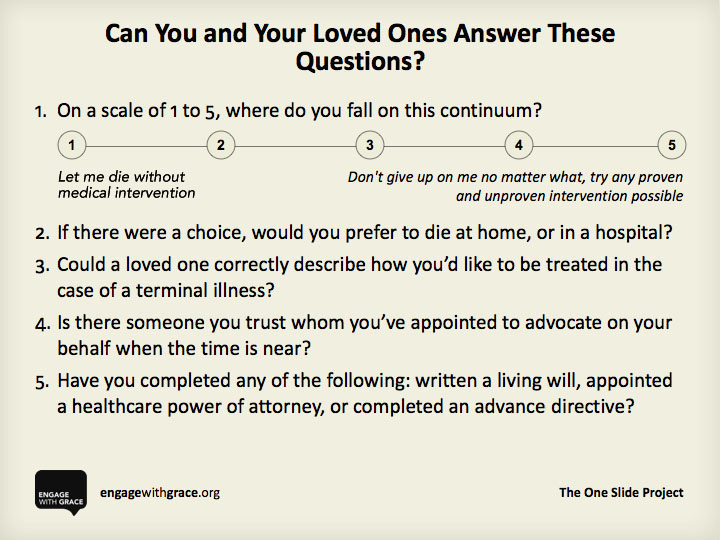
Engage with grace blog rally
This year I’m joining in the Engage With Grace blog rally. For three years running now, a number of bloggers have participated in a “blog rally” to promote Engage With Grace – a movement aimed at making sure all of us understand, communicate, and have honored our end-of-life wishes. The rally coincides with a weekend when many of us in the United States are celebrating Thanksgiving and are with close friends and family.
At the heart of Engage With Grace are five questions designed to get the conversation about end-of-life started.
To learn more please go to www.engagewithgrace.org

UK group will challenge “CAM” misinformation
I am alerted by Dr. Stephen Barrett’s Consumer Health Digest that a new UK-based group, The Nightingale Collaboration, has been launched by Simon Singh, Alan Henness, and Maria MacLachlan. The group’s website states that “The Nightingale Collaboration will work to improve the protection of the public by ensuring claims made about complementary and alternative therapies are not misleading.” The group will do this by:
- challenging misleading claims made by practitioners on their websites, in advertisements and in their promotional and sales materials and subjecting these to scrutiny by the appropriate regulatory bodies;
- striving to ensure that organizations representing complementary and alternative practitioners have robust codes of conduct for their members that protect the public and that these are rigorously enforced.
Sounds promising. I’m going to be following this new initiative. The group can be followed on Twitter @NightingaleC.

{kind=link}