Blog Archives
More data on alirocumab and diabetes risk
I happened to see an abstract from the American Heart Association Scientific Sessions in which the authors slice and dice the alirocumab data to see if they could find effects on development of diabetes or impaired glucose control in patients without diabetes at baseline. As you can see in the table below, there are some numerical differences in (1) patients with normal blood sugar at baseline who developed impaired glucose control and (2) patients with impaired glucose control who developed diabetes. The differences were not statistically significant. No resolution of this issue is likely until the results of the outcomes trials are available. See my previous post on this here.

Do PCSK9 inhibitors affect diabetes risk?
Two PCSK9 inhibitors, evolocumab and alirocumab, are under consideration at the FDA and will be the subject of advisory committee meetings on June 9 and 10. Evolocumab and alirocumab are monoclonal antibodies that inhibit proprotein convertase subtilisin/kexin type 9 (PCSK9), an enzyme that plays a role in regulating levels of LDL cholesterol by binding to LDL receptors and promoting their degradation; the resulting reduction in LDL receptors reduces the liver’s ability to remove circulating LDL. PCSK9 inhibitors prevent PCSK9 from degrading LDL receptors; the increased LDL receptor density results in increased clearance of LDL from the bloodstream. The expectation is that lower LDL levels in patients who receive PCSK9 inhibitors will result in a reduction in cardiovascular events and this strategy is currently being tested in large outcomes trials, which will be completed in a few years. Until those trials are completed, the safety and efficacy of these drugs will not be known.
One of the unknowns with PCSK9 inhibitors is their effect (if any) on blood glucose levels and the development of new-onset diabetes. Statins are known to increase the risk of new-onset diabetes by about 9% overall, with increased risk from intensive vs. moderate intensity statin therapy. One reason to wonder whether PCSK9 inhibitors might have a similar effect is that both statins and PCSK9 inhibitors, though having different mechanisms of action, both involve the removal of LDL through upregulation of LDL receptors. The reason statins increase blood glucose is unknown, but recently it has been suggested that that the LDL receptor might be involved, with greater LDL receptor activity correlating with a higher risk of diabetes. A recent study showed that patients with familial hypercholesterolemia (FH) in the Dutch FH registry have a lower prevalence of type 2 diabetes as compared to their unaffected relatives. FH is a genetic disease in which the LDL receptor function is reduced, leading to higher serum levels of LDL cholesterol. In addition, the study found a dose-response relationship, with more severe FH mutations linked to lower risk of diabetes as compared to less severe mutations. In other words, the study showed an association between less functional LDL receptors and a lower prevalence of type 2 diabetes. In an editorial, David Preiss and Naveed Sattar note that the study suggests that “the expression and function of LDL receptors may be important for glucose homeostasis” and that the advent of PCSK9 inhibitors provides an opportunity to further examine a possible link between LDL receptor expression and glycemia and diabetes risk.
I’ve looked at some of the published data on PCSK9 inhibitors and blood glucose and diabetes risk. With respect to alirocumab, I abstracted a subset of the data in an abstract presented at the March 2015 American College of Cardiology conference.
As you can see, the data show small numerical increases in new-onset diabetes and worsening of preexisting diabetes, as well as larger increases in fasting glucose and hemoglobin A1c over the course of a year in patients on alirocumab as compared to patients on placebo (all patients were also on a statin). With respect to evolocumab, I found the following data:
1. A 52-week placebo-controlled trial of evolocumab in patients with hyperlipidemia published in the New England Journal of Medicine in 2014 found the mean change from baseline for fasting glucose at week 52 was 1.3 mg per deciliter for evolocumab and 0.4 mg per deciliter for placebo. The mean change from baseline for HbA1c at week 52 was 0.02% for evolocumab and 0.00% for placebo (table 3 and supplementary table S3).
1. The Osler trials recently published in the New England Journal of Medicine showed that 1.1% of the patients who received evolocumab developed diabetes, as compared to 0.7% of the patients in the standard of care group.
What do all these small differences add up to? It’s not possible to say yet, but I assume someone will do a meta-analysis at some point, and there may be some discussion of this issue in the FDA review of these agents, which will be posted prior to advisory committee meetings.
I should note that even if PCSK9 inhibitors do increase blood glucose and the risk of developing diabetes, they would still be very worthwhile for patients who are at significant risk of heart attack and stroke, if they are shown to be effective and have acceptable safety.
American Heart Association journal announces new Patient Viewpoints
The following is reposted from e-patients.net.
The American Heart Association journal Circulation: Cardiovascular Quality and Outcomes has announced a new Patient or Caregiver Viewpoint section in the journal. Viewpoints will be authored by patients or their caregivers and will discuss the patient’s experience of heart disease, stroke, or other cardiovascular disease and their interactions with the healthcare system.
As Harlan Krumholz and I explain in an Editor’s Note, the editors of the journal hope that Viewpoints “will contain insights from the patient’s perspective along with suggestions on how to improve clinical care and healthcare delivery.”
The first Viewpoint, by a heart disease patient, discusses how he experienced interactions with his physicians over whether he should start a blood pressure medication and his thoughts on how physicians and patients could work together in a manner consistent with the patient’s values and goals.
Viewpoints will contain a minimum of medical jargon and will be freely accessible to the public. The journal hopes to make these articles a regular feature. If you are a patient living with or at risk of cardiovascular disease, or a friend or family member of such a patient, please consider submitting a Viewpoint. Instructions for authors are posted on the journal’s website.
Input needed on stent decision aid
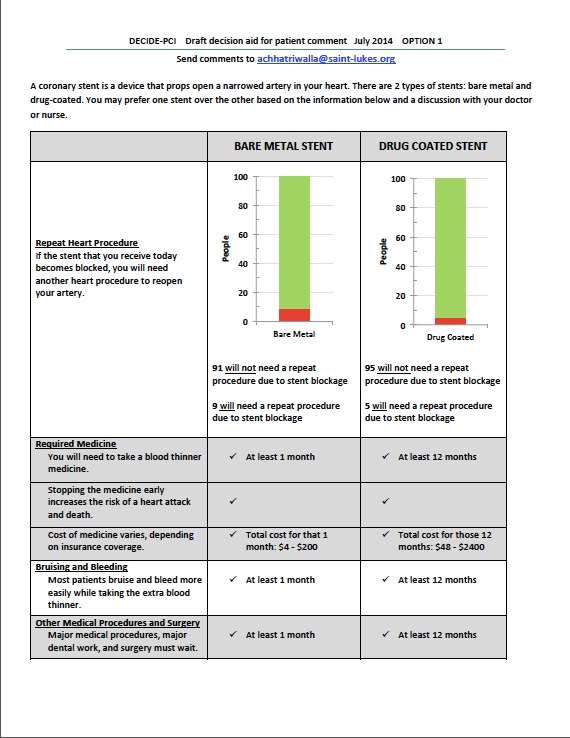
I have a post up on e-patients.net (the Society for Participatory Medicine blog) discussing a draft decision aid that some PCORI-funded researchers are developing to help patients choose between bare metal stents and drug-eluting stents. Here’s an excerpt:
The study is in the beginning phase, and the researchers are engaging patients in focus groups to better understand what factors are most important to them in choosing a stent. The focus groups will also involve asking patients how they prefer the information to be presented (e.g., in words, graphs, some combination of the two, and so forth). Later, the decision aid will be tested at two hospitals to see if it improves patient understanding and satisfaction, and if the use of the decision aid changes the percentages of bare metal stents and drug-eluting stents received by the patients.
Dr. Chhatriwalla is very interested in getting feedback from patients and others on the current drafts of the decision aid (two different versions) and has asked SPM to help circulate them. You do not need to be a heart disease patient to participate — the researchers are interested in a wide range of viewpoints. Please take a look at both of them (posted below) and send your comments to Dr. Chhatriwalla at achhatriwalla@saint-lukes.org.
(Click to enlarge.)

Perspective in Circulation: Cardiovascular Quality and Outcomes
Recently, I joined the editorial board of Circulation: Cardiovascular Quality and Outcomes, the American Heart Association journal that focuses on quality of care and outcomes research. As my readers know, I became interested in cardiovascular disease because my daughter has heterozygous familial hypercholesterolemia, a genetic disease that cause high LDL-cholesterol and can lead to premature heart disease. I wrote this perspective for the November issue on how engaged patients can help bring about positive change in health care.
Compare and contrast: two review articles on ezetimibe
For the past several years I have been following the ezetimibe controversy (see these posts on Gooznews and this blog here, here, here, here, here, here, here, here, here, here, here, here, here, here, and here). In my view, we continue to lack evidence of ezetimibe’s clinical benefit, or even safety, 10 years after FDA approval.
I have a Google Scholar Alert for ezetimibe, so often links to articles on ezetimibe arrive in my email inbox. Recently, two review articles on ezetimibe were published that were a study in contrasts. The first, by Sheila Doggrell, takes a skeptical view toward ezetimibe and reaches the following conclusion:
The comparison of clinical trials with simvastatin and ezetimibe alone and together has clearly shown that simvastatin decreases LDL-cholesterol and this is associated with improved clinical outcomes. Also, ezetimibe alone or in the presence of simvastatin lowers LDL-cholesterol. However, ezetimibe alone or in the presence of simvastatin has not been shown to have any irrefutable beneficial effects on clinical outcomes. Thus, until/unless the use of ezetimibe is clearly shown to improve clinical outcomes, its use should be largely restricted to clinical trials investigating clinical outcomes, and ezetimibe should not be used routinely in everyday practice.
The second, by Binh An Phan, Thomas Dayspring and Peter Toth, takes a much more optimistic view:
In the current treatment of cardiovascular disease, many subjects fail to reach LDL-C targets or remain at high risk for CHD events despite optimal statin and medical therapy. Ezetimibe inhibits intestinal cholesterol absorption and is effective in lowering cholesterol as monotherapy or in combination with statins in several populations, including those with FH, sitosterolemia, and insulin resistance. Significant controversy has been generated regarding the clinical effectiveness of ezetimibe, particularly after the publication of ENHANCE and ARBITER-6 despite both trials having significant methodological flaws that limited their ability to evaluate the benefit of ezetimibe. Growing data suggest that ezetimibe in combination with statin has a positive effect on the progression of atherosclerosis and reduces cardiovascular events in subjects at risk for CHD, including those with chronic kidney disease. Results from IMPROVE-IT are forthcoming and may help to guide better the use of ezetimibe in very high-risk CHD populations. Until that time and based upon the current available data, ezetimibe should remain a viable adjunct to statin therapy in the treatment of hypercholesterolemia.
Dr. Phan and colleagues find reasons to dismiss the negative results of ENHANCE and ARBITER 6-HALTS as due to “methodological flaws” and use copious amounts of hand-waving to find support for ezetimibe in the SEAS and SHARP trials, even though those trials compared the combination of simvastatin and ezetimibe with placebo and thus can tell us nothing about what, if anything, ezetimibe added to those results. Could the differing views of Doggrell and Phan et al. have anything to do with the fact that Dr. Doggrell declares no conflicts of interest relating to ezetimibe, while Phan, Dayspring and Toth declare the following conflicts:
Binh An Phan is a speaker for Abbott. Thomas Dayspring consults for Abbott, GSK, Health Diagnostic Labs, Kowa Company, Eli Lilly, Merck, Genentech, The Roche Group, Genzyme, and Omthera. He is on the Lecture Bureau for Abbott, GSK, Health Diagnostic Labs, Kowa, Eli Lilly, LipoScience, Merck. Peter P Toth is a speaker for Abbott, AstraZeneca, Amylin, Boehringer-Ingelheim, GSK, Kowa, Merck and consults for Abbott, Aegerion, AstraZeneca, Atherotech, Genzyme, Genentech, Kowa, and Merck.
It is not too surprising that authors who are consultants and on the speaker’s bureau for Merck would take a favorable view of ezetimibe. What is surprising is that anyone would take their word for it.
References
Doggrell SA. The ezetimibe controversy — can this be resolved by comparing the clinical trials with simvastatin and ezetimibe alone and together? Expert Opin. Pharmacother. (2012) 13(10):1469-1480.
Phan BAP, et al. Ezetimibe therapy: mechanism of action and clinical update. Vascular Health and Risk Management 2012:8:415-427.
Addendum, May 5, 2015: Unfortunately, the GoozNews blog is no longer up on the web.
Hayward and Krumholz: Open Letter to the Adult Treatment Panel IV of the National Institutes of Health
Rodney Hayward and Harlan Krumholz have published an open letter to the committee that is currently engaged in writing updated guidelines for cardiovascular risk reduction. Their letter challenges the committee to replace the current “treat to target” paradigm with a “tailored treatment” approach, as discussed below.
The primary focus of the current set of guidelines, ATP III , was a strategy of treating patients to target LDL-cholesterol levels, known as the “treat to target” paradigm. Moreover, the “cutpoints,” or triggers, for initiating therapy are also based on LDL levels, with higher risk patients having lower cutpoints. However, as Hayward, Krumholz and colleagues have previously argued (see here, here and here), the treat to target paradigm was not based on the results of clinical trials, since no major randomized controlled trial has tested the benefits of treating patients to LDL targets. Rather, the trials have used fixed doses of lipid-lowering drugs.
Hayward and Krumholz argue that LDL levels are not particularly useful in assessing the 2 factors that help determine the benefit of a treatment for an individual patient: (1) risk of morbidity and mortality in the absence of treatment (baseline risk) and (2) the degree to which the treatment reduces that risk. For calculating baseline risk, LDL is only one of several factors that are considered, including age, gender, smoking, blood pressure, HDL, and family history of premature cardiovascular disease and in most cases contributes little to the estimate of cardiovascular risk. For the second factor, clinical trials of statins demonstrate that the relative benefits of statins are not substantially related to pretreatment LDL levels. Thus, a high risk person may have low LDL levels and a low risk person may have high LDL levels and the high risk person will derive more absolute benefit more from treatment even though his or her LDL is low (illustrated in this table).
Hayward and Krumholz also argue that treating to LDL targets can lead to treatments that have not been shown to be safe. The treat to target approach can mean initiating treatment in patients at a relatively young age, leading to potentially many years of statin treatment. The long-term safety of this approach is not yet known. In addition, the perceived need to reach an LDL target often leads to the addition of nonstatin drugs such as niacin and ezetimibe when the maximum dose of a statin is reached and the patient’s LDL is still above goal. The benefit and safety of adding these drugs on top of statin therapy has not yet been demonstrated.
The “tailored treatment” approach Hayward and Krumholz advocate bases intensity of statin treatment on a person’s 5- or 10-year cardiovascular risk. In a previous paper, Hayward et al. tested a tailored treatment model of primary prevention using 5-year coronary artery disease (CAD) risk and compared it with the treat to target approach. In their model, a person with 5% to 15% risk would be prescribed 40 mg simvastatin and a person with greater than 15% risk would be prescribed 40 mg atorvastatin. Using this simulated model, the tailored treatment approach was found to prevent more CAD events while treating fewer persons with high-dose statins as compared to the treat to target approach.
For the reasons stated above, the tailored treatment approach does appear to me to be superior to the treat to target approach. At the same time, I note that the decision to take a statin is a personal decision. For primary prevention, the absolute benefit for most people of taking a statin over a 5 or 10 year period is small. Each person should calculate their baseline risk (there are online risk calculators for this), look at how much their risk can be lowered with a statin, and ask themselves if the benefit seems worth it to them in terms of cost, inconvenience and possible side effects (including a small increase in risk of developing diabetes).
In addition, I note that neither approach is designed to apply to patients with heterozygous familial hypercholesterolemia (FH). Due to the very high risk of premature coronary heart disease in FH patients (approximately 85% of male FH patients and 50% of female FH patients will suffer a coronary event by age 65 if untreated), the treatment paradigm for FH patients is that all are treated with statins starting in childhood or early adulthood (not everyone agrees that it is necessary to start treatment in childhood but that’s a topic for another day). In other words, FH patients are treated based on their lifetime risk, not their 5- or 10-year risk.
References
Hayward RA, Krumholz HM. Three reasons to abandon low-density lipoprotein targets: an open letter to the Adult Treatment Panel IV of the National Institutes of Health. Circ Cardiovasc Qual Outcomes. 2012:5;2-5.
Hayward RA, Hofer TP, Vijan S. Narrative review: lack of evidence for recommended low-density lipoprotein treatment targets: a solvable problem. Ann Intern Med. 2006;145:520-530.
Krumholz HM, Hayward RA. Shifting views on lipid lowering therapy. BMJ. 2010;341:c3531.
Hayward RA, Krumholz HM, Zulman DM, Timbie JW, Vijan S. Optimizing statin treatment for primary prevention of coronary artery disease. Ann Intern Med. 2010;152:69-77.
Rind DM. Intensity of lipid lowering therapy in secondary prevention of coronary heart disease. In: Freeman MW, Sokol HN, eds. UpToDate. 19.3 ed.
Chantix meta-analysis
Because I was on vacation when the latest Chantix (varenicline) news broke, I’m a week late in posting on it. Last Monday, a meta-analysis was published online in the Canadian Medical Association Journal. The meta-analysis, which combined 14 Chantix clinical trials involving 8216 partcipants, showed a 72% increased risk of ischemic or arrhythmic adverse cardiovascular events. Moreover, all except one trial involving approximately 700 participants excluded patients with a history of cardiovascular disease, indicating that Chantix may have heart risks even for people without a history of heart trouble. The meta-analysis follows last month’s FDA warning that Chantix may raise the risk of cardiovascular events in persons with a history of cardiovascular disease.
A number of people have raised safety concerns with Chantix since it was approved in 2006, including John Spangler and Curt Furberg of Wake Forest University School of Medicine (see background here, here and here), both of whom were co-authors on the meta-analysis. In 2008, researchers at the Institute for Safe Medication Practices issued a report showing a high rate of serious adverse events associated with the drug. In response to the ISMP report, the Federal Aviation Administration said it would no longer permit pilots or air traffic controllers to use Chantix, and the Federal Motor Carrier Safety Administration advised medical examiners to not qualify anyone currently using Chantix for a commercial motor vehicle license. The Chantix label includes a warning that Chantix may impair driving ability. The label also contains a boxed warning relating to Chantix’s psychiatric risks. Last year, a study published in The Annals of Pharmacotherapy found that Chantix was associated with violent or aggressive thoughts and acts. A study in PLoS One found that Chantix was associated with acts of violence toward others.
In my opinion, smokers should rely on other methods to stop smoking, such as nicotine replacement therapy, bupropion or counseling, rather than using Chantix.
