Blog Archives
National Physicians Alliance conference
In past years I have attended the NPA annual conference. I didn’t make it this year, but I want to share some projects that were discussed there that I learned about from an email from Jean Silver-Isenstadt, NPA executive director.
- “Just Price” — This project would pilot methods for physicians to assess patients’ financial vulnerability; collect and publish local price data from hospitals, pharmacies, and area providers for 50-100 of the most common diagnostic procedures and treatments; and promote discussion of diagnosis and treatment costs as part of informed, shared decision-making. The publication of transparent price lists by some in the health sector would create marketplace pressure for all to be as forthcoming.
- “There’s Safety in the Conversation” — Building on the soon-to-be-released TandemHealth app, this project would support physician-patient shared decision-making based on conflict-free, evidence-based guidelines to reduce overtreatment and waste while promoting patient safety. The project would promote a model policy of safe-haven from malpractice lawsuits specifically for episodes of care in which these conversations were documented.
- “Fair Bargain” — This project would put pressure on non-profit hospitals to deliver on the community benefit required in exchange for maintaining tax-exempt status. A new robust scorecard would compare hospital expenditures, quality of community health needs assessments, and degree of consumer and physician involvement in decision-making. Public scorecards have a track record of creating transformative pressure on institutions.
The TandemHealth app is a joint project of Consumer Reports and NPA. It is designed to be used before, during and after the clinical encounter and will present evidence-based information on common medical conditions.
These projects all sound pretty interesting. You can follow NPA on Twitter or visit the NPA website to learn more.
American Heart Association journal announces new Patient Viewpoints
The following is reposted from e-patients.net.
The American Heart Association journal Circulation: Cardiovascular Quality and Outcomes has announced a new Patient or Caregiver Viewpoint section in the journal. Viewpoints will be authored by patients or their caregivers and will discuss the patient’s experience of heart disease, stroke, or other cardiovascular disease and their interactions with the healthcare system.
As Harlan Krumholz and I explain in an Editor’s Note, the editors of the journal hope that Viewpoints “will contain insights from the patient’s perspective along with suggestions on how to improve clinical care and healthcare delivery.”
The first Viewpoint, by a heart disease patient, discusses how he experienced interactions with his physicians over whether he should start a blood pressure medication and his thoughts on how physicians and patients could work together in a manner consistent with the patient’s values and goals.
Viewpoints will contain a minimum of medical jargon and will be freely accessible to the public. The journal hopes to make these articles a regular feature. If you are a patient living with or at risk of cardiovascular disease, or a friend or family member of such a patient, please consider submitting a Viewpoint. Instructions for authors are posted on the journal’s website.
Input needed on stent decision aid
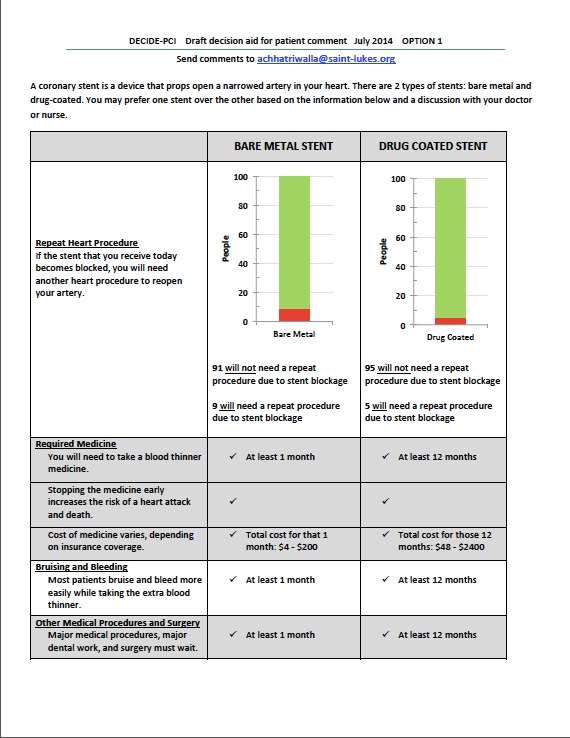
I have a post up on e-patients.net (the Society for Participatory Medicine blog) discussing a draft decision aid that some PCORI-funded researchers are developing to help patients choose between bare metal stents and drug-eluting stents. Here’s an excerpt:
The study is in the beginning phase, and the researchers are engaging patients in focus groups to better understand what factors are most important to them in choosing a stent. The focus groups will also involve asking patients how they prefer the information to be presented (e.g., in words, graphs, some combination of the two, and so forth). Later, the decision aid will be tested at two hospitals to see if it improves patient understanding and satisfaction, and if the use of the decision aid changes the percentages of bare metal stents and drug-eluting stents received by the patients.
Dr. Chhatriwalla is very interested in getting feedback from patients and others on the current drafts of the decision aid (two different versions) and has asked SPM to help circulate them. You do not need to be a heart disease patient to participate — the researchers are interested in a wide range of viewpoints. Please take a look at both of them (posted below) and send your comments to Dr. Chhatriwalla at achhatriwalla@saint-lukes.org.
(Click to enlarge.)

Making health care more patient-centered
I have a post up on the Assessment 2020 blog on how to increase patient involvement in medical decision making. I focus on shared decision making and argue that physicians need to develop certain competencies in order for the use of shared decision making to become routine and how certain structural changes can facilitate the process. Please read and add your comment!
My new Walking Gallery jacket
https://twitter.com/ReginaHolliday/status/454373909647720448
Welcome to #theWalkingGallery @MarilynMann with your jacket “Shared Decision Making.” pic.twitter.com/P3XeE07QbZ
— Regina Holliday (@ReginaHolliday) April 10, 2014
Thank you Regina Holliday, for painting this beautiful jacket!
10 steps to better risk communication
Every day, patients are faced with difficult medical decisions. These decisions invariably involve tradeoffs between risks and benefits. However, these risks and benefits are often not communicated in a way the patient can understand, if they are communicated at all. In a commentary in the Journal of the National Cancer Institute, Angela Fagerlin and colleagues highlight 10 methods that have been shown to improve understanding of risk and benefit information. Their commentary uses examples relating to cancer screening, prevention, and treatment, but the principles should apply in other areas. Below I summarize the key points; the authors state that the first three recommendations are based on strong evidence, while the rest are based on preliminary evidence.
- Communicate using “plain language.” According to the authors, the average American reads at an 8th grade level, but health education materials are often written at a high school or college level, making the information hard for the average person to understand.
- Present statistical information using absolute risk rather than using relative risk or number needed to treat formats. Changes in risk appear larger when presented using relative risk rather than absolute risk. Absolute risk is easier for most people to understand than number needed to treat.
- Use pictographs when possible when presenting information graphical format. The authors state that pictographs are easier to understand than other types of graphs, such as bar graphs and pie charts.
- Present data using frequencies rather than percentages. “10% of patients get a bad rash” and “10 out of a hundred patients get a bad rash” mean the same thing, but percentages are more abstract and/or harder to understand for some people.
- When discussing treatment complications or side effects, differentiate between baseline risks and incremental risks. Baseline risks are risks the person would face without any treatment; incremental risks are the risks associated with treatment. For example, an initial pictograph could show baseline risk and a second pictograph could add a new color to represent the additional people who would experience the side effect as a result of the treatment.
- Be aware that the order of presenting risks and benefits can alter risk perceptions. For example, if the benefits are presented first and the risks second, the risks may be perceived to be more worrisome and common. This issue can’t be avoided altogether, but can be minimized by summarizing all the information at the end.
- When there are numerous risks and benefits, use a summary table. Many treatments have numerous risks and benefits. It is easier to compare the risks and benefits if they are presented in a summary table.
- Recognize that comparative risk information can bias decision making by altering how a person views his or her own risk. If a person is given information indicating that their risk of developing a disease is higher than average, they may be more likely decide in favor of an intervention. Decisions should be based on whether the benefits of the intervention outweigh its risks for an individual person, which can only be decided based on absolute risk.
- Consider that providing less information may be more effective. Presenting more information can distract people from focusing on the key pieces of information that are needed for decision making.
- Make clear the time interval over which a risk occurs (e.g., 5-year risk, 10-year risk, 20-year risk).
I recommend reading the entire commentary. If you don’t have access to the PDF, email me and I will send it to you.
