Thoughts on the recent PCSK9 inhibitor studies
Two studies on the PCSK9 inhibitors evolocumab and alirocumab were recently published in the New England Journal of Medicine (see here and here). See this story by Larry Husten for the details. Evolocumab and alirocumab are monoclonal antibodies that are in development and are seeking FDA approval based on LDL-cholesterol reduction this year. The two studies were not designed to answer the question of whether evolocumab and alirocumab prevent cardiovascular events. Rather, the studies measured LDL reduction and tabulated adverse events over a 52- or 78-week time period. Among the adverse events being tabulated were cardiovascular events and there were fewer cardiovascular events in the patients who were in the evolocumab and alirocumab groups, as compared to patients who received placebo or usual care. One of the studies had prespecified an exploratory analysis of cardiovascular events. For the other study the investigators did a post hoc analysis of certain cardiovascular events. Neither study was powered (i.e., big and long enough) to provide a reliable estimate of the benefits of these drugs in reducing heart attacks, strokes and deaths. In other words, statistically speaking the studies were pretty thin gruel and the companies as well as the investigators acknowledge that fact. So, as of now, we really do not know that these drugs reduce the risk of cardiovascular events, let alone by how much. Nor do we really know how safe the drugs are. All these studies tell us is that as of now these drugs appear to be progressing satisfactorily along the path to approval and we just have to be patient for a couple of years until the results of the outcomes trials are available.
Fortunately, the sponsors have started large cardiovascular outcomes trials in high risk patients (e.g., the alirocumab trial will involve 18,000 patients and a minimum of 1613 primary endpoint events and a minimum two year followup — see here for a description of the trial).
I suggest taking a look at this short video of Harlan Krumholz speaking from the conference — I completely agree with his comments (website registration may be required). I also agree with the editorial by Donald Lloyd-Jones and Neil Stone, in which they state:
The ODYSSEY LONG TERM and OSLER studies whet our appetites for further results that show cardiovascular benefit and documented safety, even at substantially lower LDL cholesterol ranges than achieved before. However, it would be premature to endorse these drugs for widespread use before the ongoing randomized trials, appropriately powered for primary end-point analysis and safety assessment, are available. Reports from several lipid treatment trials provide important object lessons in this regard. Two trials of niacin revealed lower levels of LDL cholesterol and lipoprotein(a) when niacin was added to statin therapy but no net clinical benefit and very worrisome signals of harm. A randomized, controlled trial of torcetrapib reminds us that “off-target” effects can scuttle a promising drug. And the recent long-awaited presentation of results of a trial in which ezetimibe was added to moderate-intensity statin therapy in high-risk patients showed only modest benefit, though with excellent safety.
Advertising LVADs
Advanced heart failure is a debilitating and lifethreatening disease that has become increasingly common as our population ages. Patients who have reached a point where their disease threatens their survival are not always candidates for heart transplantation. Even for those that are, only a limited number of donor hearts are available. In the last two decades, implantable pumps to supplement the heart’s function have become available. A left ventricular assist device (LVAD) is a mechanical pump that is implanted in heart failure patients to help the heart’s left ventricle pump blood throughout the body. An LVAD can be used as either a “bridge-to-transplant” to help a patient survive until a donor heart becomes available, or as “destination therapy,” to provide long-term support in patients who are not candidates for a transplant. An LVAD can in some cases prolong the life of heart failure patients whose symptoms can no longer be controlled with medications.
As with any other medical intervention, there are risks and burdens associated with LVAD implantation. The medical risks of the procedure include bleeding, development of blood clots, infection, respiratory failure, kidney failure, stroke, and device failure. LVAD patients must be connected to electricity at all times and are advised not to drive. Each LVAD patient must have a dedicated caregiver to assist with batteries, changing dressings, transportation, and activities of daily living. Heart failure patients often suffer from other medical problems that are not alleviated by LVAD placement. Quite a bit of emotional stress and in some cases financial stress is involved. In addition to heart failure cardiologists and cardiac surgeons, social workers and in some cases bioethicists and palliative medicine specialists meet with the patient to ensure that he or she understands the risks, benefits and alternatives to device placement. The patient must be in a position to make a well-informed decision as to whether to have an LVAD implanted, and it is not uncommon for patients to decline the procedure.
It must be recognized that cardiac surgery, including LVAD implantation, is big business for many medical centers. I was reminded of this when I received the Fall 2014 edition of Center Scope, the newsletter sent to patients and former patients of Medstar Washington Hospital Center (WHC), Washington, DC. I have embedded the newsletter below. The cover story focuses on a 66-year-old patient named Alberto Gomez, who received an LVAD at Washington Hospital Center. Mr. Gomez appears to be a somewhat atypical patient, in that he had enjoyed excellent health up until suddenly developing extreme fatigue and being diagnosed with advanced heart failure. In any case, Mr. Gomez seems to be a great guy, and I want to make clear that I do not intend to criticize him at all. Rather, my beef is with the way the public affairs & marketing department of WHC, which produces Center Scope, has used Mr. Gomez’s story to spin a happy tale in which “hope,” “determination,” and “faith” are the only things a person needs to manage serious illness.
Alberto’s mental strength and determination served him well. He did not need a blood transfusion during surgery, an often needed measure, and declined pain medication in recovery. And when a stroke he suffered after discharge initially left him with weakness and speech deficits, Alberto overcame them with hard work and perseverance. Currently, Alberto is on a transplant list for a new heart, which doesn’t stop him from living life. “I stay very busy,” he shares. “And I have no time for complaining.”
While Alberto’s heart now requires a LVAD to ensure proper function, his heart needs no assistance in dispensing generosity, kindness and faith. Since recovering from surgery, Alberto has made it a priority to return to the Hospital Center to visit with patients facing similar procedures. “I share my experiences,” Alberto says. “I pray with them and I cry with them. I tell them to trust in the doctors and the technology.”
I’m very glad that Mr. Gomez is doing well. However, I couldn’t help thinking that the message (from WHC, not Mr. Gomez) that a positive attitude can conquer all is a bit insulting to the many LVAD patients who don’t do well. Were their complications — or their need for pain medication — due to lack of determination?
At the end of the story is the following sentence: “For more information on our heart failure services, visit MedStarHeartInstitute.org/Trust.” I thought to myself that even though the story consisted of one long human interest anecdote, at least at this link I can find some more objective information. On going to the indicated webpage, however, I was disappointed to find only a shortened version of Mr. Gomez’s story and a link to the full version. (The WHC website does have some information on heart failure and LVADs, but I had to click around a bit in order to find it.) I get that hospitals want to advertise their services, but my message for Washington Hospital Center is, how about a little more objective information and a little less schmaltz.
IMPROVE-IT trial
The long-awaited IMPROVE-IT trial was presented last month at the American Heart Association Scientific Sessions. Here are the presentation slides:
IMPROVE-IT was a trial that tested the ability of ezetimibe (Zetia) to lower the risk of heart attacks and strokes when added to simvastatin. See Larry Husten’s background post here, and if you type “ezetimibe” in the search box on this blog or on the Gooznews blog, you will find some previous posts of mine relating to ezetimibe. I admit I was a bit surprised that the trial was positive. I was expecting it to be negative, based on the negative results of the ENHANCE trial. Still, the benefit was small, a 6.4% reduction in risk of the primary endpoint (composed of cardiovascular death, heart attack, unstable angina requiring hospitalization, coronary revascularization, and stroke). In the high-risk trial participants — all patients who had been hospitalized for acute coronary syndrome within the 10 days before randomization — this translated to a 2% absolute benefit over 7 years. Of note, there was no reduction in all-cause or cardiovascular mortality.
I only want to make a few comments now, but I intend to write more when the trial is published. First, a 6.4% reduction is risk is a very small benefit, and many people would only consider that reduction in risk meaningful in a high risk population. Second, it is regrettable that we had to wait 12 years after the drug’s approval to find out whether it improves outcomes.
Here are great summaries by Larry Husten and Matt Herper. And here is a video of Harlan Krumholz giving his take on the results.
Addendum, May 5, 2015: Unfortunately, the GoozNews blog is no longer up on the web. I asked Merrill Goozner what happened and he said he decided to stop paying the annual fee for the website. So the posts I wrote on ezetimibe for GoozNews are no longer up.
National Physicians Alliance conference
In past years I have attended the NPA annual conference. I didn’t make it this year, but I want to share some projects that were discussed there that I learned about from an email from Jean Silver-Isenstadt, NPA executive director.
- “Just Price” — This project would pilot methods for physicians to assess patients’ financial vulnerability; collect and publish local price data from hospitals, pharmacies, and area providers for 50-100 of the most common diagnostic procedures and treatments; and promote discussion of diagnosis and treatment costs as part of informed, shared decision-making. The publication of transparent price lists by some in the health sector would create marketplace pressure for all to be as forthcoming.
- “There’s Safety in the Conversation” — Building on the soon-to-be-released TandemHealth app, this project would support physician-patient shared decision-making based on conflict-free, evidence-based guidelines to reduce overtreatment and waste while promoting patient safety. The project would promote a model policy of safe-haven from malpractice lawsuits specifically for episodes of care in which these conversations were documented.
- “Fair Bargain” — This project would put pressure on non-profit hospitals to deliver on the community benefit required in exchange for maintaining tax-exempt status. A new robust scorecard would compare hospital expenditures, quality of community health needs assessments, and degree of consumer and physician involvement in decision-making. Public scorecards have a track record of creating transformative pressure on institutions.
The TandemHealth app is a joint project of Consumer Reports and NPA. It is designed to be used before, during and after the clinical encounter and will present evidence-based information on common medical conditions.
These projects all sound pretty interesting. You can follow NPA on Twitter or visit the NPA website to learn more.
American Heart Association journal announces new Patient Viewpoints
The following is reposted from e-patients.net.
The American Heart Association journal Circulation: Cardiovascular Quality and Outcomes has announced a new Patient or Caregiver Viewpoint section in the journal. Viewpoints will be authored by patients or their caregivers and will discuss the patient’s experience of heart disease, stroke, or other cardiovascular disease and their interactions with the healthcare system.
As Harlan Krumholz and I explain in an Editor’s Note, the editors of the journal hope that Viewpoints “will contain insights from the patient’s perspective along with suggestions on how to improve clinical care and healthcare delivery.”
The first Viewpoint, by a heart disease patient, discusses how he experienced interactions with his physicians over whether he should start a blood pressure medication and his thoughts on how physicians and patients could work together in a manner consistent with the patient’s values and goals.
Viewpoints will contain a minimum of medical jargon and will be freely accessible to the public. The journal hopes to make these articles a regular feature. If you are a patient living with or at risk of cardiovascular disease, or a friend or family member of such a patient, please consider submitting a Viewpoint. Instructions for authors are posted on the journal’s website.
Input needed on stent decision aid
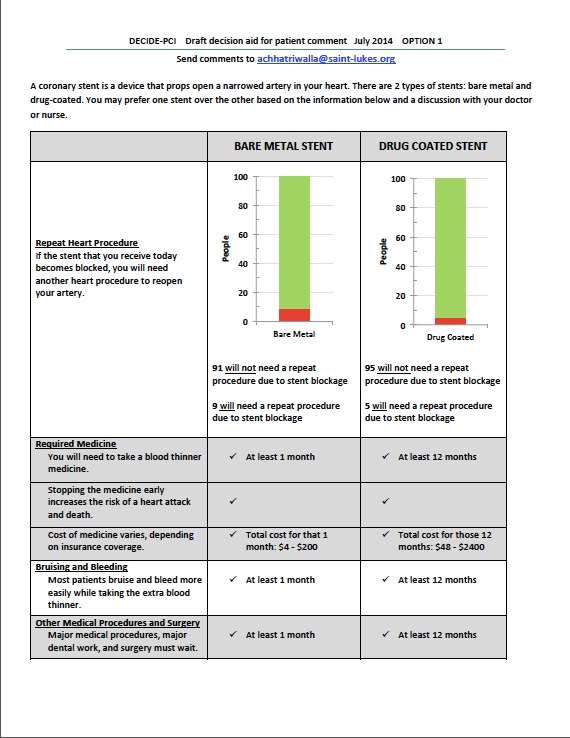
I have a post up on e-patients.net (the Society for Participatory Medicine blog) discussing a draft decision aid that some PCORI-funded researchers are developing to help patients choose between bare metal stents and drug-eluting stents. Here’s an excerpt:
The study is in the beginning phase, and the researchers are engaging patients in focus groups to better understand what factors are most important to them in choosing a stent. The focus groups will also involve asking patients how they prefer the information to be presented (e.g., in words, graphs, some combination of the two, and so forth). Later, the decision aid will be tested at two hospitals to see if it improves patient understanding and satisfaction, and if the use of the decision aid changes the percentages of bare metal stents and drug-eluting stents received by the patients.
Dr. Chhatriwalla is very interested in getting feedback from patients and others on the current drafts of the decision aid (two different versions) and has asked SPM to help circulate them. You do not need to be a heart disease patient to participate — the researchers are interested in a wide range of viewpoints. Please take a look at both of them (posted below) and send your comments to Dr. Chhatriwalla at achhatriwalla@saint-lukes.org.
(Click to enlarge.)

Making health care more patient-centered
I have a post up on the Assessment 2020 blog on how to increase patient involvement in medical decision making. I focus on shared decision making and argue that physicians need to develop certain competencies in order for the use of shared decision making to become routine and how certain structural changes can facilitate the process. Please read and add your comment!
My new Walking Gallery jacket
https://twitter.com/ReginaHolliday/status/454373909647720448
Welcome to #theWalkingGallery @MarilynMann with your jacket “Shared Decision Making.” pic.twitter.com/P3XeE07QbZ
— Regina Holliday (@ReginaHolliday) April 10, 2014
Thank you Regina Holliday, for painting this beautiful jacket!
New series of articles in Circulation: Cardiovascular Quality and Outcomes
Circulation: Cardiovascular Quality and Outcomes will be publishing a new series of articles called narratives, which will be written by patients or by their family, friends or caregivers.
Narratives: The purpose of this series is to further understanding of patients’ experience of cardiovascular disease. These articles will be written by patients, or by their family members, caregivers, or friends. The articles will explore the effects of illness and treatment on patients’ lives and on their relationships with family, friends, caregivers, and health care providers. They will often discuss aspects of a condition that are important to patients but may not be fully appreciated by clinicians. We are especially interested in publishing narratives that contain lessons on the strengths and weaknesses of our health care system. They may, for example, be designed to help health care providers become aware of problems in communication of information, decision making, care coordination, access, cost, timeliness, safety, equity, and quality of care.
More information is available here. Submit your article here.
